Why I Left Clinical Work for Partnerships — and What I Miss

I trained to counsel patients.
Now I write proposals.
That's the shortest possible version of my career so far, and the version most colleagues at Kenyatta National Hospital would not have predicted from the first-year intern who would not stop talking about complementary feeding.
This is the longer version. The version I owe my younger self, my younger colleagues, and the patient I never got to follow up.
Table of Contents
- Why I Studied Nutrition
- The Patient I Still Think About
- What "Partnerships" Actually Means
- What I Gained
- What I Lost
- What I'd Tell A Younger Me
- Why I'm Telling You This
Why I Studied Nutrition
I was the kid who asked too many questions about food. My grandmother would patiently answer most of them and then send me away to fetch sukuma. I am from a family where food is care. My mother feeds people the way other parents say "I love you."
I went to Kenyatta University to do Food, Nutrition and Dietetics because I wanted the precision behind the love. I wanted to know — actually know — why ugali and beans satisfies a child for four hours and bread and tea satisfies them for one. I wanted the science of the kitchen.
The lectures delivered, mostly. The clinical placements delivered, painfully.

The Patient I Still Think About
In my fourth year I did a placement in a county hospital. There was a six-month-old with severe acute malnutrition. The mother had walked five hours to get there. Her older child had died of similar complications eighteen months earlier. The chart still said follow-up overdue.
We stabilised the baby. We sent the mother home with F-100, a feeding plan, and a follow-up appointment. She missed the follow-up. The clinic had no transport budget to find her. I checked the records six weeks later. Nothing.
I went home that night and sat on my bed for an hour without taking off my shoes. I had done my job. The system had not done its job. The baby was somewhere I could not see.
That was the moment I realised I would not survive thirty years on the bedside side of this work without breaking. And I started reading about systems.

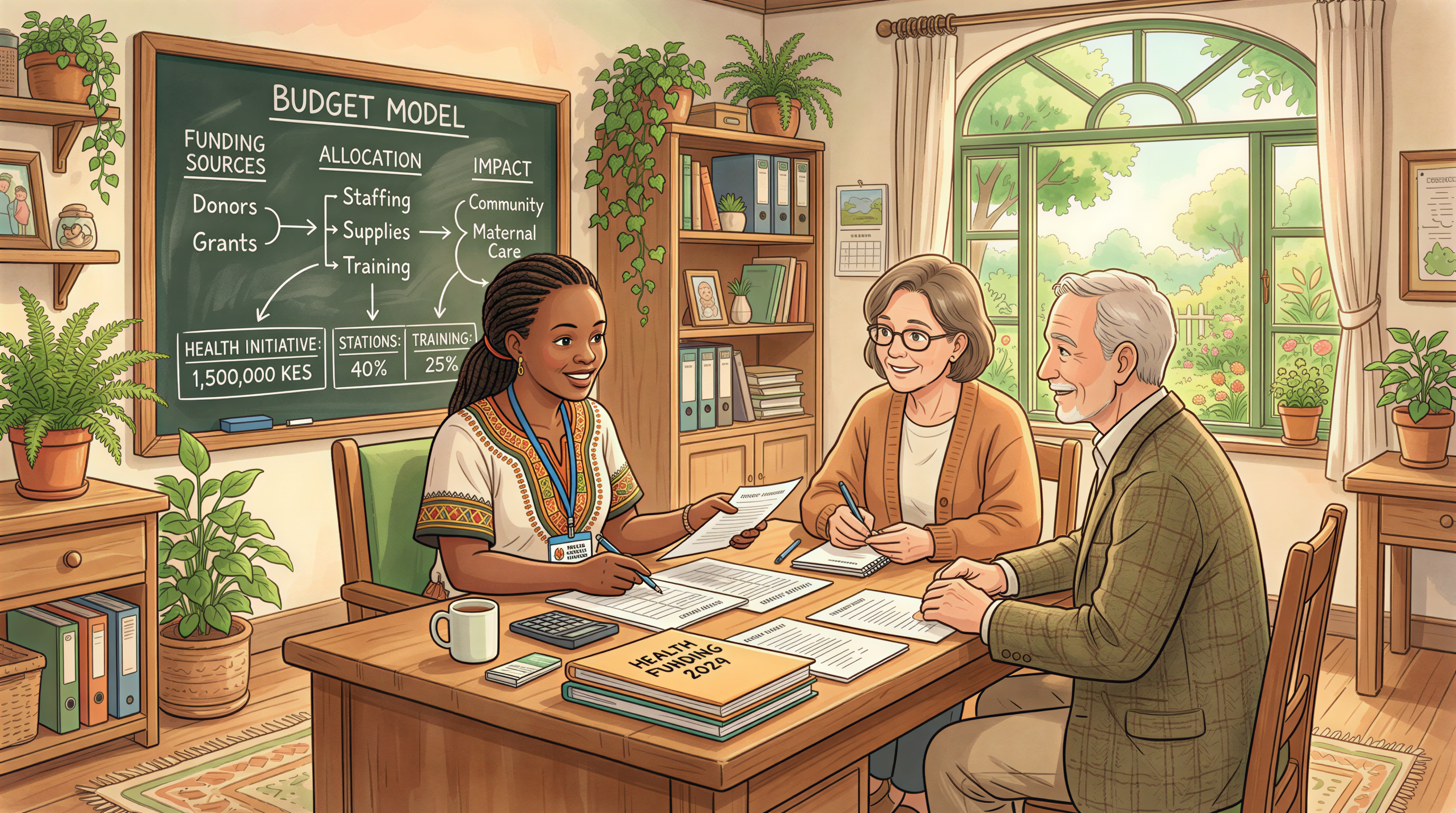
What "Partnerships" Actually Means
Most people outside the NGO world think "partnerships" is a vague title. It is not. The job, in plain terms, is:
- Funding. Reading donor calls, interpreting them honestly, deciding which ones are worth applying to.
- Proposal writing. Translating frontline reality into a budget, a logframe, and a theory of change a donor can fund.
- Government relations. Sitting in meetings with the Ministry of Health, the National Treasury, county departments. Understanding what is policy, what is performance, and what is just political weather.
- Reporting. Translating field results back into language that survives a donor's compliance review.
- Saying no. Turning down funding that would distort the program, turning down partnerships that exist mostly for the partner's logo.
It is interpretive work. It is also where the leverage sits. A good proposal moves more food onto more plates than a clinician can in a year. A bad one moves nothing — or worse, moves the program in a direction the field never asked for.
What I Gained
Three things.
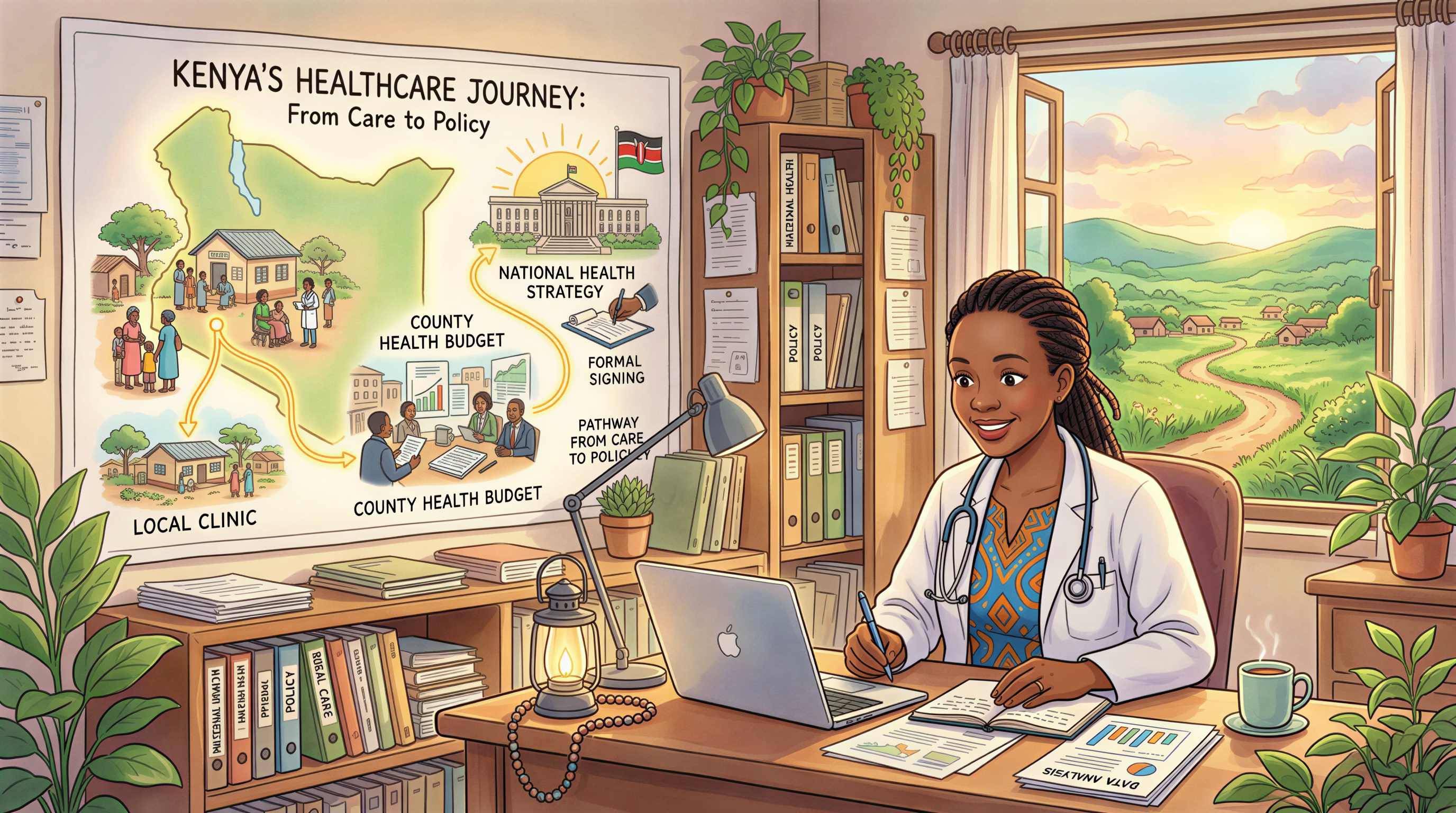
1. A wider field of view.
The bedside view is intense and intimate. The system view is wider and more honest. Sitting at my desk now, I can see the line from a Kakamega household's plate to a county nutrition budget to a national strategy to a global donor's annual report. That line was always there. I just couldn't see it from the clinic.
2. The ability to actually move money.
I have helped move tens of millions of shillings of donor funding into real programs. Each shilling moved is a meal, a CHV trained, a fortified plate, a child weighed. I think about this when I miss the bedside. The bedside multiplied is the proposal that funds twenty bedsides.
3. Better instincts about what works.
You cannot write proposals for long without developing a sharp nose for which interventions are evidence-led and which are vibes-led. I am a more useful clinician now than I was at the bedside, because I have read more programs at a programmatic level than most clinicians get to.
What I Lost
Two things, honestly.
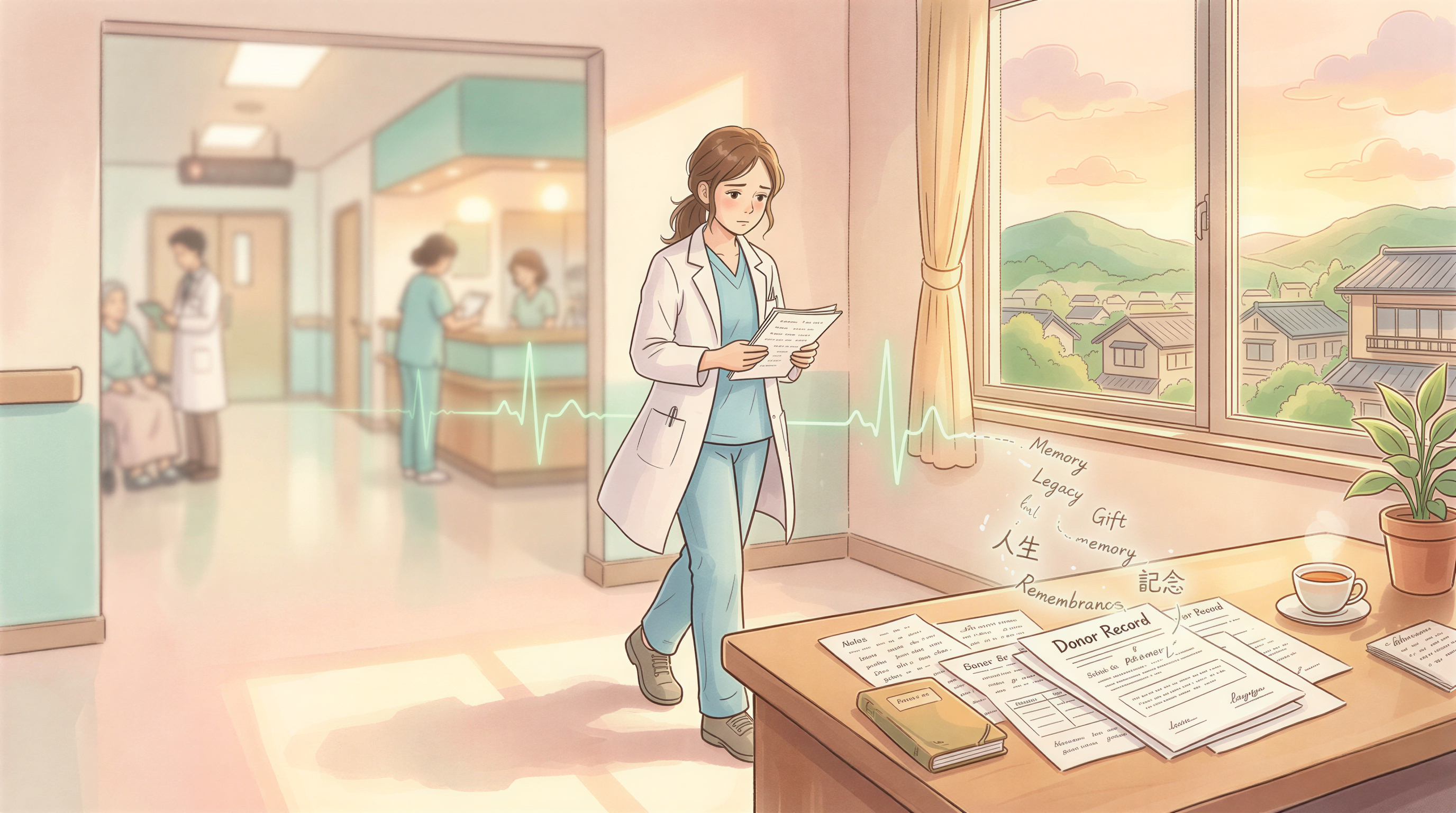
1. The patient.
Nobody calls me when their baby is recovering. Nobody updates me on the growth chart. The intimate feedback loop of clinical work — the did this work — is gone. I have to trust the field reports, the indicators, the third-party evaluations. They are good. They are not the same as a child on a scale.
I miss it. I am not romantic about it — clinical work in Kenyan public health is exhausting and underpaid — but the meaning was unambiguous. Every day I knew what I had done.
2. Some of the language.
I now write in donor English. Theory of change. Beneficiary reach. Catalytic intervention. The vocabulary is necessary inside its room and toxic outside it. I have to switch carefully when I write things like this article — and when I talk to the mother in the village. The danger is forgetting to switch back, and most of my colleagues who have done this for ten years have caught the disease at some point.
That is partly why I started this blog. The blog is a place to use the other language — the one my grandmother used. Direct. Specific. Human.
What I'd Tell A Younger Me
If I could send a note to the version of me who stayed in the car park after that placement and decided he was not going to be a clinician forever, I'd tell him:
- Don't apologise for the move. The system needs people who have stood at the bedside and sit at the desk. That is rarer than either alone.
- Keep clinical hours, even small ones. I see private clients monthly partly to stay calibrated. The day you can't read a feeding chart fluently, you are no longer translating — you are just relaying.
- Write in plain language at least once a week. The donor English will eat you if you don't.
- The patient is still the point. When the proposal stops being for the patient and starts being for the funder, change something.
I am still figuring out the rest. That's why I write.
Why I'm Telling You This
I'm telling you this because the blog is going to look different from here on out. More opinion. More personal. More commentary. Fewer how-to guides for feeding your baby — there are good people writing those, and you don't need a partnerships director writing a complementary-feeding chart.
What I can offer is a view from both ends of the ladder. The bedside I trained for. The desk I work at. The proposals I write. The donors I meet. The mother whose name I still know.
I'll keep writing about maternal nutrition and the first 1,000 days — but framed as the system I now see, not as the textbook I once memorised.
If you've been here from the beginning: thanks for staying. If you're new: welcome. The view from this side of the desk is worth the climb.